Diabetic peripheral neuropathy and gastroparesis are two common complications of diabetes that can be interconnected. As a result of high blood sugar levels damaging the nerves, diabetic peripheral neuropathy can cause pain or loss of sensation in the extremities. Similarly, gastroparesis occurs when nerve damage affects the stomach muscles, leading to delayed gastric emptying and digestive issues. These two conditions may exacerbate each other, as poor blood sugar control can worsen both neuropathy and gastroparesis symptoms. It's crucial for diabetics to maintain good blood sugar levels and follow their doctor's advice to reduce the risk of these complications.
Diabetic Peripheral Neuropathy: what it feels like and how to manage it
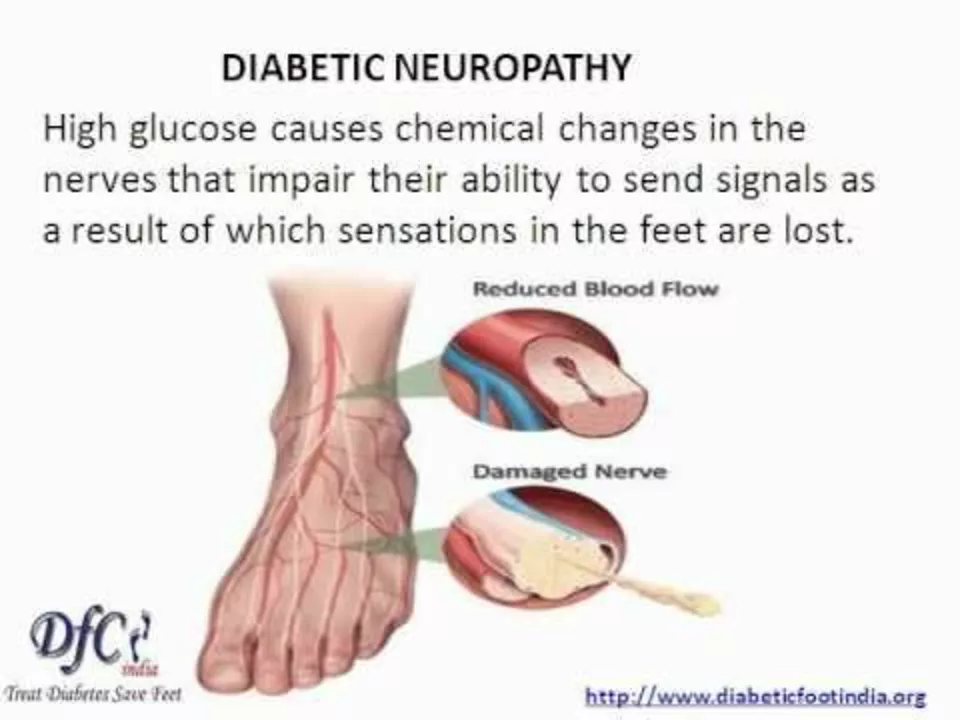
Diabetic peripheral neuropathy (DPN) is nerve damage from long-term high blood sugar that usually hits the feet first. You may notice numbness, tingling, burning, stabbing pains, or a loss of balance. Some people have more sensitivity to touch or pain that wakes them at night. Because feeling is reduced, small cuts or blisters can be missed and turn into bigger problems fast.
Why it happens and who’s at risk
High glucose levels damage small blood vessels and nerves over time. The longer you’ve had diabetes and the less controlled your blood sugar is, the higher the risk. Other factors that raise risk: high blood pressure, obesity, smoking, kidney problems, and long use of certain meds. Checking and improving these areas slows damage and lowers the chance of new nerve loss.
Start with better glucose control. Even modest drops in average blood sugar reduce stress on nerves. Work with your care team to set realistic A1c goals, and treat other risks like high blood pressure and high cholesterol.
Practical steps you can take every day
Check your feet every day. Look for redness, cuts, swelling, blisters, or changes in skin color. Use a mirror or ask for help if you can’t see the soles. Wear supportive, well-fitting shoes and never walk barefoot. Trim toenails straight across and keep skin moisturized, but don’t put lotion between toes.
For pain, common options include gabapentin, pregabalin, duloxetine, and tricyclic antidepressants such as amitriptyline. Topical choices—capsaicin cream or lidocaine patches—can help with fewer systemic side effects. Over-the-counter painkillers rarely fix neuropathic pain. Always talk to your provider about side effects and interactions before starting medication.
Non-drug measures help too: physical therapy, balance training, low-impact exercise, weight loss, and quitting smoking. TENS (electrical stimulation) gives relief for some people. If you’re on metformin, ask about checking vitamin B12—low B12 can make neuropathy worse.
Protect your feet to avoid ulcers and infections. If a sore or wound appears and doesn’t start improving in a few days, see your doctor or a podiatrist right away. Annual foot exams with simple tests for protective sensation should be part of your diabetes checkups.
Set realistic expectations: treatments often reduce pain but may not fully restore feeling. Managing DPN works best when your primary care doctor, diabetes specialist, podiatrist, and sometimes a pain specialist coordinate care. Keep a short symptom diary—what time pain hits, what makes it better or worse—so appointments are more productive.
If you notice new numbness, worsening pain, cuts that won’t heal, or balance problems, contact your healthcare provider. Simple daily habits—better glucose control, regular foot checks, sensible shoes—cut risks and keep you moving safely.




