
Ever wonder why your prescription for a generic drug is covered, but another one isn’t? It’s not random. Insurance companies don’t pick which generics to cover based on luck, brand deals, or gut feeling. There’s a strict, data-driven system behind it - and if you’re paying for meds, you need to understand how it works.
It Starts With the FDA’s Green Light
Before an insurer even looks at a generic drug, it has to be approved by the FDA. That means the generic has to contain the same active ingredient, in the same strength and dosage form, as the brand-name version. It also has to prove it works the same way in the body. The FDA doesn’t just approve it on paper - they test for bioequivalence. If a generic doesn’t deliver the same amount of medicine into your bloodstream as the brand, it gets rejected. No exceptions.Once that’s done, the drug enters the insurer’s radar. But here’s the catch: not every FDA-approved generic gets covered. Insurers don’t cover every single one. They pick the ones that make the most sense - and that’s where the Pharmacy & Therapeutics (P&T) committee comes in.
The P&T Committee: The Real Decision-Makers
Every major insurer - whether it’s Medicare Part D, UnitedHealthcare, Cigna, or Blue Cross - has a committee made up of pharmacists, doctors, and sometimes even patient advocates. This group meets regularly to review which drugs get added to the formulary. Their job? To balance three things: safety, effectiveness, and cost.They start with clinical evidence. Did the drug work in real studies? Does it have fewer side effects than others in its class? Then they look at safety history. Has this generic been on the market for years with a clean record? Or are there reports of inconsistent quality from the manufacturer? Finally, they compare prices. If two generics do the exact same thing, but one costs 30% less, the cheaper one wins. It’s not about brand loyalty. It’s about value.
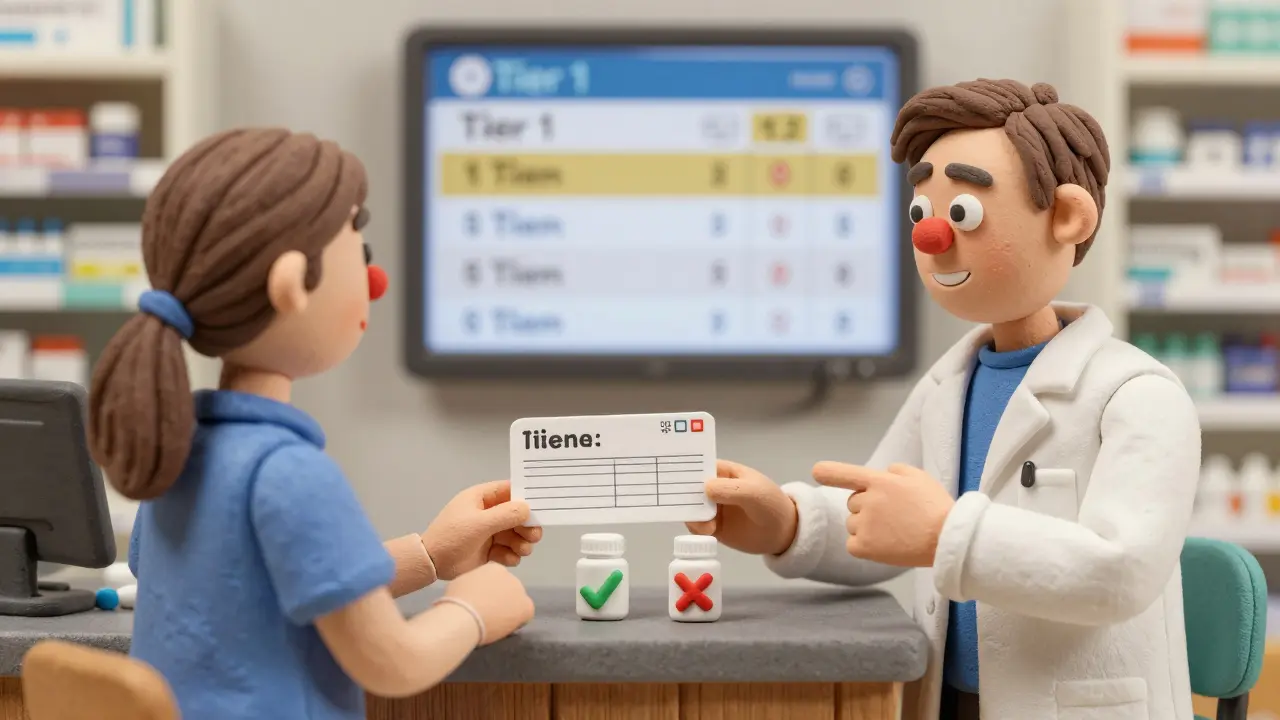
According to CMS data from 2023, 92% of Medicare Part D plans put generics in Tier 1 - the lowest cost tier. That means you pay as little as $0 to $15 for a 30-day supply. Compare that to brand-name drugs in Tier 3 or 4, which can cost $40 to $100 or more. The math is simple: generics save money. And insurers save $141 billion a year just from generic use, according to KFF analysis. That’s not charity. It’s strategy.
Tiered Formularies: How Your Drug Gets Ranked
Insurers organize drugs into tiers. Think of it like a pricing ladder. The lower the tier, the less you pay.- Tier 1: Preferred generics - these are the cheapest, most commonly used, and always covered with minimal copay.
- Tier 2: Non-preferred generics - still generic, but maybe less commonly used or slightly more expensive. You pay a bit more.
- Tier 3: Preferred brand-name drugs - higher cost, but still covered with a higher copay.
- Tier 4: Non-preferred brands - expensive, often require prior authorization.
- Tier 5: Specialty drugs - high-cost, complex medications, like those for cancer or MS.
Most generics land in Tier 1. But even within Tier 1, insurers can pick which generics they prefer. For example, if two generics for high blood pressure are equally effective, but one comes from a manufacturer that offers a bulk discount, that’s the one you’ll get. It’s not about quality - it’s about contract negotiations.
Why Some Generics Get Left Out
You might be surprised to learn that not every generic for a drug is covered. Take levothyroxine, a common thyroid medication. There are dozens of generic versions on the market. But insurers typically only cover one or two - the ones with the best track record for consistency. Why? Because even small differences in absorption can cause problems. A patient switching between generics might feel jittery, tired, or gain weight. Insurers know this. So they stick with the ones proven to be stable across batches.Another reason a generic might be excluded: it’s not cost-effective compared to another. For example, if a newer generic costs the same as an older one but offers no clinical advantage, the older one stays on the list. The system rewards efficiency, not novelty.
Therapeutic Substitution: When Your Doctor Doesn’t Get a Say
Here’s where things get tricky. In 78% of commercial plans, pharmacies are allowed to substitute a generic for a brand-name drug - even if your doctor didn’t prescribe it that way. This is called therapeutic substitution. It’s legal, it’s common, and it’s built into the formulary.But it’s not always smooth. A 2023 Drug Topics survey found that 31% of patients reported side effects after being switched to a different generic. One woman in Birmingham told her pharmacist she’d been on the same generic for seven years, then got a new bottle that made her dizzy. She went back to her doctor, who had to write a letter to the insurer explaining why the original one worked. That process took five days.
Insurers don’t always make it easy. While Medicare Advantage plans require a doctor’s approval for substitution, many private insurers let pharmacists swap drugs automatically. That’s why it’s important to ask your pharmacist: “Is this the same one I’ve been taking?”

What You Can Do When a Drug Isn’t Covered
If your generic isn’t on the formulary, you’re not stuck. You can request an exception. All insurers are required to have a process for this.Your doctor needs to submit documentation showing that:
- The drug you need causes harmful side effects,
- A similar drug didn’t work for you,
- Or you need a higher dose than the plan allows.
By law, insurers must respond within three business days. If they don’t answer? The request is automatically approved. In 2023, 78% of patients who appealed a denial eventually got coverage. That’s not a fluke - it’s policy.
But here’s the catch: it takes time. Physicians spend an average of 13.3 hours a week just dealing with prior authorizations and exceptions. That’s time they’re not spending with patients. And if your insurer has poor formulary transparency - like some regional plans that score under 2.5 out of 5 - you’re more likely to get caught in the middle.
What’s Changing in 2025 and Beyond
The rules are shifting. Starting in 2025, Medicare Part D will cap out-of-pocket drug costs at $2,000 a year. That means insurers will have to work harder to keep total spending low. Expect more focus on high-volume generics - the kind used by millions, like metformin, atorvastatin, and lisinopril.The FDA is also speeding up approvals. Under the 2023 Generic Drug User Fee Amendments, approval times are dropping from 42 months to under 10 months. That means more generics will hit the market - and insurers will have to decide which ones to cover.
But challenges remain. As of October 2023, 78% of the 372 active drug shortages in the U.S. were generics. When a manufacturer can’t keep up, insurers scramble to find alternatives - sometimes switching patients mid-treatment. That’s not ideal. And as AI-driven personalized generics emerge, insurers are unsure how to evaluate them. One P&T chair told a 2023 survey: “We don’t know how to price something that’s made for one person.”
What You Should Know
- Generics are cheaper because they’re the same drug - not a cheaper version. They’re not “second best.” - Your insurer picks generics based on proven safety, effectiveness, and cost - not because they’re paid to. - If a generic isn’t covered, you can appeal. It works more often than you think. - Always ask your pharmacist if your generic is the same one you’ve taken before. - Don’t assume all generics for the same drug are equal. Some have better consistency than others.The system isn’t perfect. But it’s designed to help you get the medicine you need at a price you can afford. Understanding how it works gives you power - not just as a patient, but as someone who’s paying for healthcare.





Jonathan Rutter
Let me tell you something nobody else will: insurers don’t care about your health, they care about their quarterly earnings. I’ve been on the same levothyroxine for 12 years, and last month they switched me without telling me - now I’m jittery, my heart races, and my doctor says ‘it’s the same chemical.’ Yeah, right. The active ingredient might be identical, but the fillers? The binders? The coating? Totally different. And guess who pays the price? You. Me. Millions of us. They’re playing Russian roulette with our thyroid function and calling it ‘cost-effective.’ This isn’t healthcare - it’s corporate gambling with human lives.
And don’t get me started on the P&T committees. Pharmacists and doctors? Sure, they’re on the panel. But who signs their paychecks? The insurance company. So when they say ‘clinical evidence,’ what they really mean is ‘which generic gives us the biggest rebate.’ I’ve seen the spreadsheets. I’ve seen the contracts. This system is rigged, and if you think it’s about patient care, you’re the one who’s delusional.
Jana Eiffel
While the systemic mechanics of formulary selection are indeed grounded in empirical analysis, one must not overlook the ethical underpinnings of pharmaceutical access. The reduction of human health outcomes to cost-per-milligram metrics risks the commodification of therapeutic necessity. One might argue that efficiency is a virtue; however, when patient stability - a phenomenon demonstrably sensitive to inter-batch variability in generic formulations - is sacrificed for margin optimization, we confront not merely a policy failure, but a moral one.
Moreover, the implicit assumption that bioequivalence equates to therapeutic equivalence, while statistically valid in aggregate populations, fails to account for individual pharmacodynamic variance. The human body is not a homogenous variable. To treat it as such is to misunderstand both physiology and dignity.
aine power
It’s not rocket science. Cheaper one wins. End of story.
Robin bremer
bro i just got switched to a new generic for my blood pressure med and i felt like i was gonna pass out for 3 days 😭
pharmacist was like ‘it’s the same thing lol’
no it’s not. my body knows. my brain knows. my anxiety knows.
why do they do this?? i’m not a lab rat 🤬
also why do i have to beg for my own medicine?? like come on.
Ashley Paashuis
Thank you for this detailed breakdown. It’s important to understand that the formulary system is designed to maximize value, not to penalize patients - though the execution often falls short. The tiered structure, while impersonal, does serve a purpose: it encourages the use of clinically effective, low-cost options that benefit the broader population.
That said, the lack of transparency around manufacturer contracts and the absence of patient input in P&T decisions remain significant gaps. I encourage anyone facing formulary denials to document everything - side effects, dosage changes, even journal entries about how you feel. These become powerful evidence when filing an exception. You are not powerless. The system is flawed, but it is not inflexible.
Arshdeep Singh
yo in india we got generics for like 5 bucks and they work fine. why is america so messed up? you guys pay 20x more for the same pill and then complain? this is what happens when you let corporations run healthcare. we have 100+ manufacturers making levothyroxine here and no one dies from switching. maybe your bodies are too soft? or maybe you’re just used to being overcharged?
also why do you think your doctor knows better? they don’t even know which generic you’re on half the time. you think they care? they get paid per visit, not per pill. so just shut up and take the cheap one.
Jeremy Williams
The institutional logic of formulary design is, in fact, a mirror of broader economic rationality. The P&T committee functions not as a medical body, but as a fiduciary agent of capital. Their mandate is not to heal, but to economize - and within that constraint, they perform with commendable rigor.
Yet the tragedy lies not in their methodology, but in the absence of a parallel ethical framework. When cost becomes the sole arbiter of access, we lose sight of the patient as a person, not a data point. The real failure is not the insurer’s decision - it is the societal willingness to accept such a reductionist model of care.
Maddi Barnes
Ohhhhh sweet mercy. I’ve been on the same generic for 15 years. Then last year, my pharmacy switched me ‘because it’s cheaper.’ I went from feeling like a normal human to a zombie who couldn’t wake up before noon. I had to go to my doctor, who had to write a letter, then wait 8 days for approval. Meanwhile, I was crying in the shower because I couldn’t even hold my coffee without shaking.
And guess what? The ‘cheaper’ one? It was made by a company in China that had a recall last month for inconsistent dissolution rates. So yeah. I’m glad someone finally wrote this. But can we PLEASE stop pretending this is ‘science’? It’s corporate arbitrage with my life as the currency.
Also - why is no one talking about how pharmacies get kickbacks to switch? 🤔
And to the guy who said ‘just take the cheap one’ - you’re lucky your body doesn’t scream at you. My thyroid doesn’t care about your budget. Mine does. And mine is not a suggestion.
Benjamin Fox
AMERICA IS THE BEST HEALTHCARE SYSTEM IN THE WORLD PERIOD. EVERY OTHER COUNTRY IS A SOCIALIST HELLHOLE. IF YOU CAN’T AFFORD MEDS THEN DON’T BE LAZY AND GET A BETTER JOB. WE PAY FOR YOUR PRESCRIPTIONS WITH OUR TAXES AND YOU COMPLAIN? THIS IS WHY WE CAN’T HAVE NICE THINGS. STFU AND TAKE THE GENERIC.
PS: I’M A VET AND I’VE SEEN REAL SUFFERING. YOU THINK THIS IS BAD? TRY LIVING IN AFGHANISTAN.
MAKE AMERICA GREAT AGAIN
Greg Scott
I just want to say - thank you for writing this. It’s rare to see someone explain this stuff without sounding like a corporate brochure. I’ve been through the exception process twice. It’s exhausting. But I did it. And I got my medication back. It’s not easy, but it’s possible. And if you’re reading this and you’re stuck - you’re not alone. Keep pushing. You deserve to feel like yourself again.
Davis teo
Okay but what if I’m the one who’s allergic to the filler in the ‘preferred’ generic? What if I get hives? What if I have to go to the ER? And then they say ‘oh, just switch to the other one’ - the one that’s cheaper but has a different coating that makes me feel like I’m being electrocuted from the inside?
I’ve been in this system for 10 years. I’ve called 14 different insurers. I’ve filed 7 appeals. I’ve had 3 doctors write letters. I’ve cried in 5 pharmacy waiting rooms.
And still - they act like it’s my fault for not being ‘flexible.’
My body isn’t a spreadsheet. I’m not a line item. I’m a person. And I’m tired.
Michaela Jorstad
This is such an important post. Thank you for laying it all out so clearly. I especially appreciate the note about asking your pharmacist - I didn’t realize that was a legitimate, necessary question until last year. Now I ask every single time. And yes - sometimes the pill looks different. Sometimes the name on the bottle changes. And yes - sometimes I panic. But now I know what to do.
To anyone reading this who’s scared to speak up: you have rights. You have a voice. And you’re not being ‘difficult’ for wanting to feel stable. You’re being smart. Keep going. You’ve got this.