
INR Stability Calculator
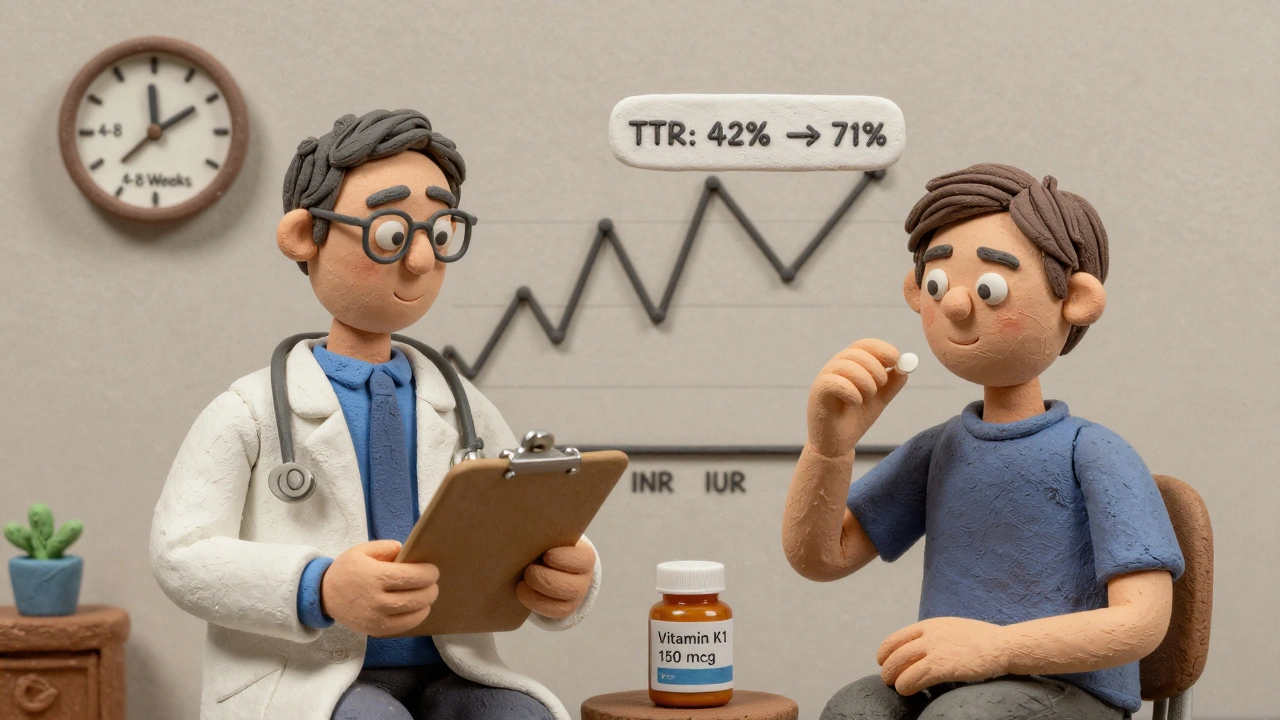
Based on clinical studies, consistent daily vitamin K intake of 150 mcg helps stabilize INR for warfarin patients. This tool estimates how your vitamin K intake affects your INR stability based on the research in the article.
For many people on warfarin, keeping their INR in range feels like walking a tightrope. One week they’re fine, the next their INR spikes to 5.0 or drops to 1.5-no clear reason why. It’s frustrating, scary, and sometimes dangerous. If you’ve been on warfarin for months or years and still can’t get stable results, even with careful dosing and diet tracking, you’re not alone. About one in three people on warfarin struggle with unpredictable INR levels. That’s where vitamin K supplements come in-not to replace warfarin, but to help make it work more smoothly.
Why Does Warfarin Make INR So Unstable?
Warfarin works by blocking vitamin K’s role in making clotting factors. But your body doesn’t get the same amount of vitamin K every day. A big salad one day, a burger the next, a multivitamin with K on Wednesday-it all throws off your INR. That’s not your fault. It’s how warfarin works. Even small changes in vitamin K intake can swing your INR out of the safe zone (2.0-3.0). For people with mechanical heart valves, the target is even higher (2.5-3.5), making stability even harder.
Research shows that people with unstable INR tend to eat far less vitamin K daily than those who stay stable. One study found unstable patients averaged just 109 micrograms of vitamin K per day, while stable ones got nearly 300. That’s a huge gap. And it’s not about eating too much or too little overall-it’s about inconsistency.
How Low-Dose Vitamin K Helps
The idea isn’t to flood your body with vitamin K. It’s to give you a steady, small amount every day-150 micrograms-so your body doesn’t have to guess. Think of it like filling a bucket with a leaky hose. If the water flow changes every hour, the level goes up and down. But if you add a slow, constant drip from another source, the level stays steady. That’s what 150 mcg of vitamin K1 does.
This dose is about 1.5 times the daily recommended amount for adults (90-120 mcg), but it’s still far below any toxic level. The European Food Safety Authority says you’d need to take over 10,000 times this amount daily to risk harm. It’s safe. And it’s cheap. A 5 mg bottle of generic vitamin K1 costs about $8 and lasts over a year at this dose.
Studies show this approach doesn’t always boost your overall Time in Therapeutic Range (TTR)-the main metric doctors use. But it does something just as important: it cuts down on dangerous spikes and drops. One major trial found patients on vitamin K had 4% fewer extreme INR readings (below 1.5 or above 4.5). That might sound small, but for someone who had 11 dangerous INRs in six months, that could drop to just 5. Fewer spikes mean fewer emergency visits, fewer dose changes, and less anxiety.
Who Should Consider Vitamin K Supplements?
This isn’t for everyone. If your INR is stable, you don’t need it. If you’ve just started warfarin, give it time. But if you’ve been on it for six months or more and your INR keeps jumping around-despite eating the same foods, taking your pill at the same time, and avoiding interactions-you might be a candidate.
Doctors typically look for these signs:
- TTR below 65% over the last 6 months
- Three or more INR values outside the target range in the past 3 months
- No clear cause for instability (like missed doses, alcohol use, or new medications)
It’s also not recommended for people with mechanical mitral valves (they need tighter control), those who’ve had recent clots or bleeding, or anyone with active cancer. If you’re on dialysis, talk to your doctor-this group often benefits the most.
What Happens When You Start?
Don’t just start taking vitamin K on your own. You need to work with your anticoagulation clinic or doctor. Here’s how it usually goes:
- They check your recent INR history to confirm instability.
- You start taking 150 mcg of vitamin K1 daily, usually as a tablet.
- You keep taking your regular warfarin dose-at first.
- For the first month, you’ll check your INR weekly. It may dip lower than usual in the first 2-4 weeks. That’s normal. Your body is adjusting.
- Your doctor will slowly increase your warfarin dose if needed. On average, people need 0.5-1.5 mg more warfarin per day after starting vitamin K.
- After the first month, INR checks usually go to every two weeks, then monthly.
It takes 4-8 weeks to see real improvement. Don’t give up if your INR is still wobbly after two weeks. This isn’t a quick fix. It’s a long-term adjustment.
What Doesn’t Work
Some people try vitamin K and it doesn’t help-or even makes things worse. That usually happens for one of three reasons:
- You’re not consistent. Taking vitamin K only when you eat greens? That defeats the purpose. It has to be daily, every day.
- You’re eating too much vitamin K. If you’re drinking kale smoothies daily or eating large amounts of natto, spinach, or broccoli, your body is already getting plenty. Adding more can backfire.
- You’re missing warfarin doses. Vitamin K won’t fix poor adherence. If you skip pills, the instability isn’t from vitamin K-it’s from you.
One case study followed a 72-year-old woman whose INR got worse after starting vitamin K. Turns out, she was taking warfarin only every other day. The vitamin K masked the problem until she had a dangerous bleed. That’s why monitoring doesn’t stop-you still need regular INR checks.
Vitamin K vs. Other Options
What about DOACs like apixaban or rivaroxaban? They don’t need INR monitoring and are easier for most people. But they’re not for everyone. If you have a mechanical heart valve, antiphospholipid syndrome, or severe kidney disease, warfarin is still the only option. That’s about 2 million people in the U.S. alone.
Point-of-care INR machines let you test at home. They’re great for quick feedback, but they cost $500-$1,000 and require training. Vitamin K doesn’t need equipment. It just needs consistency.
Some clinics now combine both: home testing + vitamin K. That’s the gold standard for high-risk patients.
What Experts Say
Doctors aren’t all on board yet. The American College of Chest Physicians says the evidence isn’t strong enough for a formal recommendation. But they also don’t say no. The European Heart Rhythm Association gives it a “may be considered” rating-Class IIb, Level B. That means: it’s not first-line, but it’s reasonable for certain patients.
Dr. Elaine Hylek from Boston University calls it “one of the most promising approaches.” Dr. Jacob Siegel at Johns Hopkins says the 4% drop in dangerous INR excursions could prevent thousands of bleeding events each year.
The big hurdle? Most doctors don’t know about it. Only 28% of U.S. anticoagulation clinics offer it as an option. But that’s rising. The American Heart Association added it as a “promising practice” in early 2023. A major trial called VIKING, expected to finish in late 2024, could change guidelines for good.

Real Stories
One man, 68, had a mechanical aortic valve. For 18 months, his INR bounced between 1.2 and 5.1. He had 17 dose changes. After starting 150 mcg vitamin K daily, his TTR jumped from 42% to 71%. He had only two dose changes in the next six months.
Another woman, on Reddit, said her TTR went from 55% to 78% after six months. “I finally slept through the night,” she wrote.
Not everyone wins. One user said his dose had to go up from 3 mg to 4.5 mg, and he wasn’t sure it was worth it. But he’s not alone. About 68% of patients who’ve tried it report better stability. Around 10% say it made things worse-usually because they weren’t consistent or had other issues.
How to Talk to Your Doctor
If you think this might help you, come prepared. Bring your INR log. Say: “I’ve been on warfarin for X months and my INR keeps swinging. I read about low-dose vitamin K helping people with unstable results. Could we consider trying it?”
Ask if your clinic has a protocol. If they say no, ask if they’d be open to reviewing the evidence. The Canadian and U.K. guidelines already acknowledge it. NICE in the UK says it can be used “on a case-by-case basis.”
Don’t buy random supplements. Get vitamin K1 (phylloquinone). Avoid K2. Don’t use multivitamins-they’re too unpredictable. Look for 150 mcg tablets. Some pharmacies stock them; others need to order them. Your clinic can help.
Final Thoughts
Vitamin K supplements aren’t magic. They won’t fix bad habits or replace careful monitoring. But for people stuck in the warfarin rollercoaster, they’re one of the few tools that actually work. It’s not about taking more clotting agents. It’s about making your body’s chemistry more predictable. That’s how you stay safe.
If you’ve been fighting your INR for years, this might be the quiet solution you’ve been waiting for. Talk to your doctor. Get your records. Give it a fair shot. Stability isn’t impossible-it just needs the right approach.





Linda Migdal
Let’s be real-this isn’t some miracle cure. It’s just biochemistry with a marketing spin. Warfarin’s instability isn’t because you skipped kale-it’s because the drug has a half-life of 40 hours and a therapeutic window thinner than a dollar bill. Adding vitamin K is like trying to stabilize a Jenga tower by gluing one block. It might look better for a while, but the structure’s still rigged. And don’t get me started on clinics that don’t offer this-they’re still stuck in the 90s.
Tommy Walton
Bro. 🤯 Imagine your body is a quantum particle and warfarin is the observer. The moment you try to measure INR, it collapses into chaos. Vitamin K? That’s not a supplement-it’s a decoherence shield. You’re not fixing diet-you’re harmonizing your molecular dance. 🌿🌀
soorya Raju
lol u guys think this is about vitamin K? nah. it's the glyphosate in your kale. the fda knows. the pharma giants paid off the doctors. they dont want you stable. they want you coming back every week for blood tests. 150mcg? try 150mg. and dont trust any 'generic' tabs-most are fake. i got mine from a guy in delhi who swears it's from the himalayas. no receipts. no lab reports. just vibes. 🌱🪄
Grant Hurley
Man I tried this last year after my INR went to 5.8 for the third time. I was terrified. Started the 150mcg daily like the post said-no skipping, no exceptions. First two weeks? My INR dropped like a rock. Thought I was gonna bleed out. But by week 5? My numbers were smoother than my morning coffee. Still check it every two weeks. Still paranoid. But now I sleep. Seriously. I slept for 7 hours straight last night. No alarms. No panic. 🙏
Nnaemeka Kingsley
Bro, this is real. I’m from Nigeria, my dad on warfarin after stroke. We didn’t even know about this until a nurse in Lagos mentioned it. We got the tablet, he took it every day, no drama. Now his INR is steady. No more hospital trips. Just one pill. Simple. Cheap. No magic. Just science. You don’t need to be smart to do this. Just consistent.
Kshitij Shah
Oh wow, so now we’re treating warfarin instability like a bad yoga class? ‘Just breathe, and take your vitamin K.’ 😏 Meanwhile, my cousin’s INR spiked because he ate a whole jar of natto and thought ‘I’m healthy now.’ Spoiler: he didn’t. Vitamin K isn’t a band-aid. It’s a band-aid with a side of math. And most people can’t do math.
Sean McCarthy
Study says 4% fewer extreme INRs. That’s 4%. Not 40%. Not 400%. 4%. That’s statistically insignificant. You’re talking about reducing 11 dangerous events to 5. That’s still 5. That’s still 5 times too many. And you’re recommending a supplement that requires daily compliance from a population that can’t even remember to take their blood pressure pills? This isn’t a solution. It’s a placebo with a price tag.
Jaswinder Singh
Y’all are overcomplicating this. I’ve been on warfarin for 12 years. My INR was all over the place. I started taking 150 mcg vitamin K1 every damn day-no excuses. No ‘I’ll take it tomorrow.’ I didn’t change my diet. I didn’t buy fancy machines. I just took the pill. Now my TTR is 82%. My doctor says I’m the most stable patient he’s ever had. It’s not magic. It’s discipline. If you can’t do that, don’t blame the medicine. Blame yourself.
Bee Floyd
I just want to say-this post was incredibly thoughtful. The way you laid out the science, the real stories, the caveats-it’s rare to see this level of care in medical advice online. I’ve been helping my mom navigate warfarin for years, and this is the first thing that made me feel hopeful, not overwhelmed. Thank you for not just dumping info, but for walking us through it like a human.
Jeremy Butler
It is imperative to underscore that the proposed intervention-namely, the adjunctive administration of phylloquinone at a dosage of 150 micrograms per diem-constitutes an off-label therapeutic strategy, the efficacy of which remains contingent upon a multitude of confounding variables, including but not limited to genetic polymorphisms in VKORC1, dietary phytonutrient interference, and hepatic metabolic variance. To suggest a universal applicability is, in the strictest sense, epistemologically unsound.
Courtney Co
Wait so you’re saying I can just take a pill and stop worrying? But what if I forget? What if I take it at night instead of morning? What if my dog eats the bottle? What if I’m on vacation and they don’t have it? What if I start bleeding and no one knows why? What if my insurance doesn’t cover it? What if my doctor says no? What if I’m not sure if I’m one of the 68%? What if I’m one of the 10% who gets worse? What if I die? WHAT IF I DIE???
Shashank Vira
Ah, the noble quest for biochemical equilibrium. A modern-day alchemist’s dream-transmuting chaos into order with a single capsule. But tell me, does the universe reward our hubris? Do the enzymes bow to our schedules? Or do they laugh, as they always have, at the mortal who believes he can outwit evolution with a 150-mcg tablet? The answer, my friends, lies not in the supplement-but in the silence between heartbeats.
Eric Vlach
Just did this last month. Took the vitamin K like they said. Didn’t change anything else. First week INR dropped to 1.8. Scared me half to death. Second week it was 2.3. Third week 2.6. Now it’s 2.4 every time. My doc raised my warfarin by 1 mg. No more panic calls. No more 3 a.m. blood tests. It’s not perfect. But it’s the first time I’ve felt like I’m not fighting my own body.
Souvik Datta
Let me share something from my clinic in Delhi. We’ve been using this protocol for three years now. Not everyone responds. But for those with mechanical valves and erratic INRs? It’s life-changing. We’ve seen TTR jump from 40% to 75% in under 12 weeks. The key? We don’t just hand out pills. We sit with patients. We track their meals. We remind them. We call them. This isn’t just medicine-it’s care. And care is what makes the difference.
Priyam Tomar
Everyone’s acting like this is some breakthrough. Newsflash: vitamin K1 has been studied since the 1980s. You’re late to the party. Also, your ‘150 mcg’ is arbitrary. Why not 100? Why not 200? Where’s the RCT with a placebo group? Where’s the long-term safety data? And why are you ignoring the fact that K1 can interfere with warfarin metabolism via CYP2C9? You’re not solving instability-you’re trading one variable for another. And you’re calling it wisdom? Pathetic.